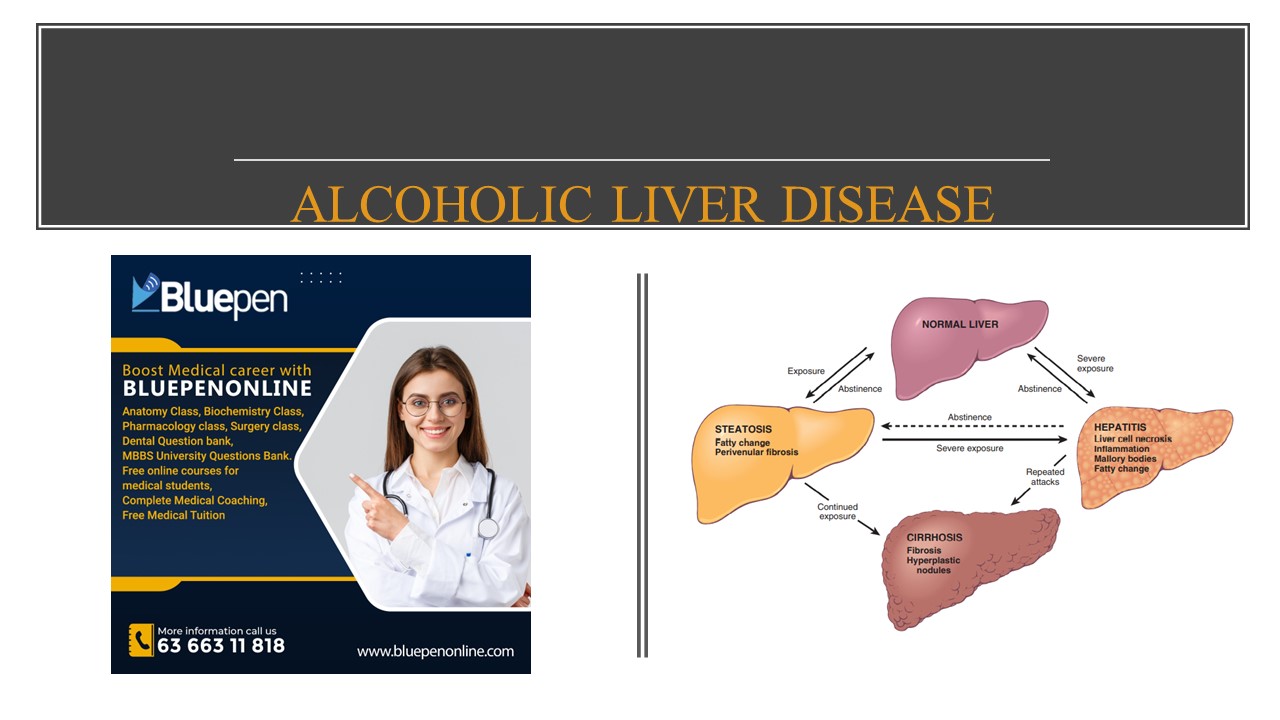
ALCOHOLIC LIVER DISEASE DOCTOR'S NOTE
Alcohol is a well-known cause of fatty liver disease in adults and can manifest histologically as
- Steatosis,
- Steatohepatitis,
- Cirrhosis
The morphological changes in alcoholic liver disease and NAFLD are indistinguishable.
MORPHOLOGY
HEPATOCELLULAR STEATOSIS
- Hepatocellular fat accumulation typically begins in centrilobular hepatocytes.
- The lipid droplets range from small (microvesicular) to large (macrovesicular),
- the lipid accumulation spreads outward from the central vein to hepatocytes in the midlobule and then the periportal regions.
STEATOHEPATITIS:
- Hepatocyte ballooning cells undergo swelling and necrosis most prominent in the centrilobular regions
- MALLORY-DENK BODIES These consist of tangled skeins of intermediate filaments
- Neutrophil infiltration. accumulate around degenerating hepatocytes, particularly those containing Mallory-Denk bodies.
STEATOFIBROSIS:
- Fibrosis appears first in the centrilobular region as central vein sclerosis.
- Perisinusoidal scarring appears next in the space of Disse of the centrilobular region
- The liver takes on a nodular, cirrhotic appearance.
PATHOGENESIS
- Short-term ingestion of as much as 80 g of ethanol per day generally produces mild reversible hepatic changes, such as the fatty liver.
- Chronic intake of 40 to 80 g/day is considered a borderline risk factor for severe injury.
COMPLICATIONS
- Hepatic failure
- Massive gastrointestinal hemorrhage
- Intercurrent infection
- Hepatorenal syndrome
- Hepatocellular carcinoma.
NAFLD
NON- ALCOHOLIC FATTY LIVER DISEASE
- NAFLD is a common condition in which fatty liver disease develops in individuals who do not drink alcohol.
- It is associated with the metabolic syndrome, obesity, type 2 diabetes, and dyslipidemia and/or hypertension.
PATHOGENESIS
- Development of obesity and insulin resistance
- Mobilization of free fatty acids from adipose tissue
- Toxic effects of inflammatory cytokines
- Increased production of reactive oxygen species, induction of ER stress, and disruption of mitochondrial function
- Stellate cell activation, collagen deposition, and hepatic fibrosis
- Full-blown NASH
CLINICAL FEATURES
- Fatigue
- Malaise
- Right upper-quadrant discomfort
- Symptoms of chronic liver disease
- Liver biopsy is required to identify NASH and distinguish it from uncomplicated NAFLD
CIRRHOSIS
MAJOR CAUSES OF CIRRHOSIS
- Chronic hepatitis B
- Chronic hepatitis C
- Non-alcoholic fatty liver disease (NAFLD)
- Alcoholic liver disease
MORPHOLOGY
- Stem cell activation and differentiation gives rise to duct-like structures, the so called ductular reactions
- In chronic liver disease, ductular reactions increase with disease progression and are usually most prominent in cirrhosis.
FEATURES OF CHRONIC LIVER FAILURE
- PRURITUS
- HYPER-ESTROGENEMIA IN MALES- spider angioma, palmar erythema, hypogonadism, gynecomastia.
- PORTAL HYPERTENSION- shunts causing multiple symptoms
- HEPATOCELLULAR CARCINOMA.
BENIGN TUMOURS OF LIVER
- Most common benign tumor of liver is the cavernous hemangioma
- Also liver can develop hepatic adenomas.
HEPATOCELLULAR CARCINOMA
ETIOPATHOGENESIS
- Chronic liver diseases are the most common setting for emergence of HCC
- The most important underlying factors in hepatocarcinogenesis are viral infections (HBV, HCV) and toxic injuries (aflatoxin, alcohol)
- Alcohol consumption with cigarette smoking
- Inherited disorders, particularly hereditary hemochromatosis and α1AT deficiency
- Metabolic syndrome, diabetes mellitus, and NAFLD
GENETIC FACTOR
Two most common driver mutations:
- Gain of function mutations in beta-catenin
- loss of function mutations in p53.
MORPHOLOGY- GROSS
- HCC may appear grossly as
1. A unifocal (usually large)
2. Multifocal, widely distributed nodules of variable size
3. A diffusely infiltrative cancer
- Vascular invasion or direct extension become more likely once tumors reach 3 cm in size
- Vascular invasion is also the most likely route for extrahepatic metastasis, especially by the hepatic venous system.
MICROSCOPY
- HCCs range from well-differentiated to highly anaplastic lesions
- Well-differentiated HCCs are composed of cells that look like normal hepatocytes and grow as thick trabeculae.
DIAGNOSIS
- Elevated serum levels of α-fetoprotein are found in 50% of individuals with advanced HCC (neither specific nor sensitive).
- Ultrasonography
- Computed tomography
- Magnetic resonance imaging.
CONSEQUENCE
DEATH usually occurs by:
- Cachexia,
- Gastrointestinal or esophageal variceal bleeding,
- Liver failure with hepatic coma,
- Rupture of the tumor with fatal hemorrhage.
TREATMENT
- Small tumors, <2cm, can be removed surgically or ablated with good outcomes.
- If relatively small HCCs arise in the setting of advanced stage (cirrhotic) chronic liver disease, liver transplantation is a better option and may be curative.
- Radiofrequency ablation and chemoembolization are used for local control of unresectable tumors.
- The kinase inhibitor SORAFENIB can prolong the life of individuals with advanced-stage HCC.
GALL STONES
PATHOGENESIS - CHOLESTEROL STONES
- Cholesterol is rendered water-soluble by aggregation with bile salts.
- When cholesterol concentrations exceed the solubilizing capacity of bile (supersaturation), cholesterol crystallizes out of the solution.
- Cholesterol gallstone formation is enhanced by hypomobility of the gallbladder (stasis), which promotes nucleation, and by mucus hypersecretion, with consequent trapping of the crystals, thereby enhancing their aggregation into stones.
PIGMENT STONES:
- Pigment stones form when the bile contains a high concentration of unconjugated bilirubin in the biliary tree,
- as may occur in patients with chronic extravascular red cell hemolysis or with certain infections of the biliary tract, such as liver flukes.
- The precipitates are primarily insoluble calcium bilirubinate salts.
MORPHOLOGY- CHOLESTEROL STONES
- Exclusively in the gallbladder and consist of 50% to 100% cholesterol.
- Pure cholesterol stones are pale yellow
- Increasing proportions of calcium carbonate, phosphates, and bilirubin impart gray-white to black discoloration
- They are ovoid and firm; they can occur singly, but most often there are several
- Most cholesterol stones are radiolucent, although as many as 20% may contain sufficient calcium carbonate to be radiopaque.
MORPHOLOGY- PIGMENT STONES
- Arise anywhere in the biliary tree and are classified into black and brownstones.
- In general, black pigment stones are found in sterile gallbladder bile, while brownstones are found in infected intrahepatic or extrahepatic ducts.
- The stones contain calcium salts of unconjugated bilirubin.
- Black stones are usually small, numerous, and fragile to the touch
- Brown stones tend to be single or few in number and to have a soft, greasy, soap-like consistency
- 50% to 75% of black stones are radiopaque
- Brownstones, which contain calcium soaps, are radiolucent.
CLINICAL FEATURES
- Asymptomatic in 70-80% of cases
- Right upper-quadrant or epigastric pain, often excruciating
- “Biliary” pain is caused by gallbladder or biliary tree obstruction or by inflammation of the gallbladder itself.
- Severe complications include empyema, perforation, fistulas, inflammation of the biliary tree, obstructive cholestasis, pancreatitis, and gallstone ileus.
.................................................................................................
Coaching for 'Mbbs Students', 'Bds Students', 'Mds Students', 'Bams Students', 'Bpt Students', 'Bhms Students', 'Nursing Students', 'PreMed Students', 'Md Students', 'Doctor Students'
Connect with Bluepenonline
"Mbbs Tuition" "Bds Tuition" "Bams Tuition" "Next Tuition" "NeetPg Tuition" "Bpt Tuition" "PreMed Tuition" "Md Tuition"v"Medical Subjects Tuition" & "Medical Lecture Notes"
Please search in google or edge as follows to connect with Bluepenonline, Find Private & Affordable MBBS Tutoring, MBBS TUTORS, Online MBBS Tuitions, online classes for mbbs students, MBBS Tuition near me, BDS Tuition, Online BDS Tuitions, BDS Tuition near me, pre-med tuitions for international students, Online BAMS tuition, BAMS Coaching classes near me, BAMS coaching classes online, Online BAMS Coaching Classes, Next/NeetPg Coaching, Ayurveda tuition, Ayurvedic medicine courses,..etc

 Common challenges faced by Ayurveda Students
Common challenges faced by Ayurveda Students Common challenges faced by BPT & Nursing Students
Common challenges faced by BPT & Nursing Students Common challenges faced by Dental Students
Common challenges faced by Dental Students Common challenges faced by MBBS Students
Common challenges faced by MBBS Students What does an MBBS student learn?
What does an MBBS student learn?